You seem to lack some knowledge about medical schools and their applications.
How so?
I’m kind of immersed in this right now as one of my children (White/Appalachian (by some definitions)) is currently applying to medical schools. So we are examining actual entrance requirements for actual real world medical schools in great detail. Including how to write essays that will help you.
I think academic ability is a better predictor of success in medicine than writing essays whose evaluation, beyond basics of proper grammar and spelling, is inherently subjective.
Medical schools *DO* have programs in the first four years of medical school that target and focus on things like primary care. It is explicit in the application process. There are seats in the medical school essentially reserved for people who will enter GP - and classes to target them.
Do you have a link to some such program? In particular, does the medical school somehow prohibit one from applying to non-primary residencies later? I know many medical schools emphasize primary care, but I know that aspiring medical students know how to play that up in essays regardless of their future plans.
You are mis-informed or using out of date information. See above.
I think you are misinformed. Specialties are a function of what residency one matches into.
See
The Match.
Many of these programs look for people who match the communities they are trying to serve,
Some explicitly say that if you must be a member of the community or have family ties to the area.
State, not "community" or "area". At least when you talk about med schools. And it is mostly public med schools that restrict eligibility to in state applicants.
So they do not call out race, but the accepted applicants will likely have a different racial make-up than the general applicant pool.
It would average out over all states though.
Both of the white people and that one Asian guy who live in rural mississippi will have a chance, of course.
Are you trying to say that there are few whites in rural Mississippi or what is your point here? Because that's not even true.
If Mr. 4.0/220 White Guy or Asian Guy answers his essay with an obvious lack of understanding of underserved communities, and an obvious lack of compelling backstory on whether they have any intention to serve those communities or capability of being comfortable in those comunities, they will lose out to someone who, perhaps with a lower GAP or MCAT, shows a willingness to serve there and compelling backstory showing they are capable of it.
When you make race part of the "backstory" then obviously you end up discriminating by race.
Here you are again conflating “URM points” with people who are admitted. The percentage of hispanic people admitted will be high, because they are more likely to know spanish. The White Appalachian who speaks spanish (such as my child - also speaks Japanese and ASL) may also get in, but she won’t be in a crowd of hundreds of Appalachian white applicants who can speak spanish, relative to the much larger number of spanish-speaking hispanic applicants.
You are missing my point. It is URM status itself that gives Hispanics and blacks points. Blacks are not likely to know Spanish either, and yet their scores and grades are even worse than for Hispanics.
Your daughter's language skills would give her a small boost over other ORMs, but it will not make up for URM status even for those who don't speak other languages.
Here’s a reason they are less likely, based on my knowledge of my Asian friends and their families: those families value education and status at a much different degree than White or Black families do. They will push their children into the most prestigious position they can. Some of my friends lament this as a real stressor in their upbringing. One friend lamented how dissappointed his parents were that he was not a cardiac surgeon but “only a thoracic surgeon”. For real.
That is wild, if true, but thoracic surgery is still a highly competitive specialty.
This is - of course - not universal of all Americans with Asian ancestry. But it is far more likely than white families, such that an Asian medical school applicant may indeed be less likely to accept long term emplyment as a GP in an underserved neighborhood.
If they match into family medicine there isn't much choice than to work as a GP. Where they work is just like for any job; it depends where you get hired. Unsurprisingly, more people regardless of race want to live in desirable cities rather than Bumfuck, Mississippi.
Yes, I meant 520. Sorry.
Pauses to laugh really hard and mutter, “220, 221, whatever it takes”.
528 or bust!
Already told you.
Asian ancestry people are a lower percent of the rural population than they are of the suburban population.
White people are less likely to have experience in diverse neighborhoods than diverse people are.
What do you mean by "diverse people"?
Why should somebody be penalized based on whether they live in a suburban or rural county? Especially when the definitions of those are fluid.
So when a medical school is selecting for people who will stick it out in those working environments for the long term, and not leave the nano-second that their residency is done, they will pick people who can demonstrate reasons that they are more likely to put down roots and stay.
Stick it out where? Close to the medical school? And why do you think blacks or Hispanics are more likely to do that?
Indeed there is certainly data about what type of people put down roots and stay in those areas. And they are not, typically, people with suburban backgrounds - who are overwhelmingly White and Asian.
Do you have those data? Because it seems to me made up to justify racial discrimination.
You assume it was done “in order to reduce the number of Asians getting accepted,” but the intent behind the measure is speculation on your part.
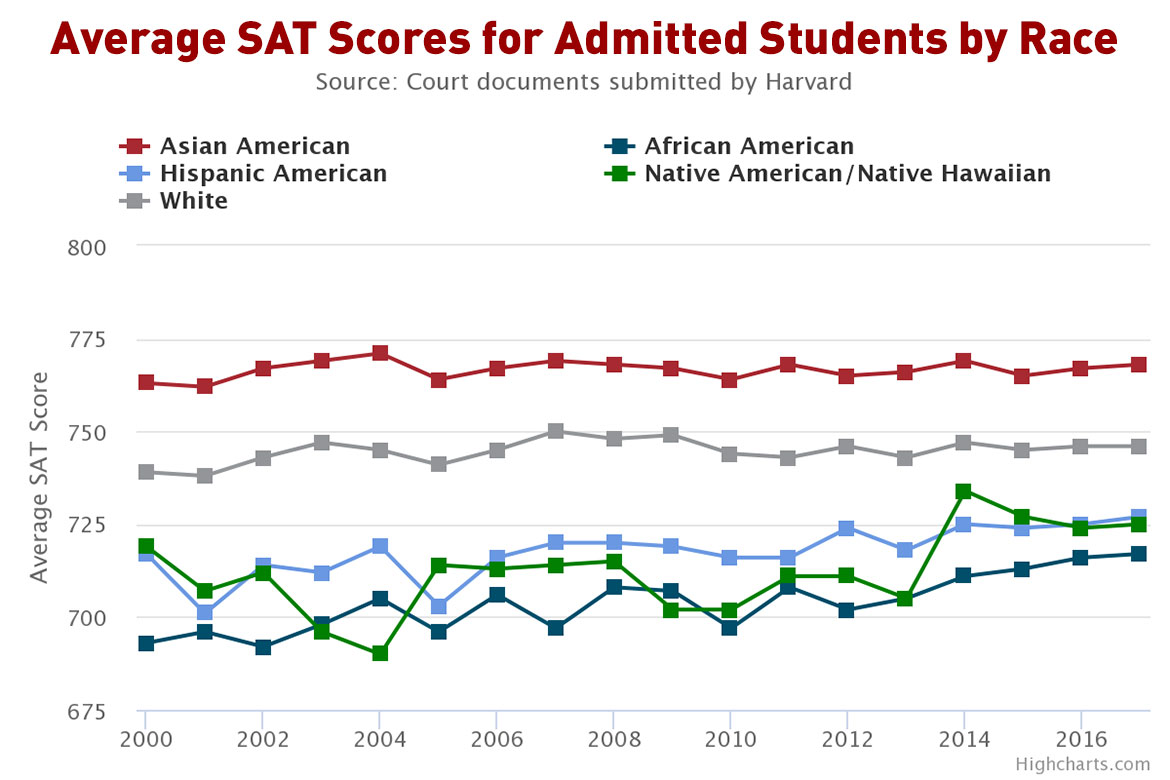
The Harvard "personality score" scandal was certainly done in order to adjust racial mix of admitted students toward fewer Asians being admitted.
Equally likely is to react to other goals such as who tends to make it through residency with favorable job reviews from their advisors. And if that does not include certain socio-economic backgrounds, that may have significantly different representations in diversity, then the “diversity” numbers will look different.
The personality score thing was for Harvard undergrad. I offered it as an example of similar shenanigans taking part outside of medical school admissions racket.
You have no reason to think you know this in order to do things racially. Maybe in some cases it is. Maybe in some cases they think, “shit, we have been discriminating against these groups for, like, ever. We have to show that we have changed, or the diverse applicants will never consider us. We have to be the change we want to see.”
Do you use "diverse" to mean "non-white"? Because that's not what the word "diverse" means.
Also, present discrimination by race is not justified by past discrimination by race. It's just perpetuating injustice.
And then they acknowledge that they will have to listen to whiners who can’t abide that they want to change fast. Wanh! No! It should be a slow curve! Only natural changes to fix artificial problems!!
Since any solution to the achievement gap starts in early childhood, it will be a slow process. Applying lower standards to certain applicants based on race and ethnicity may mask the problem, but it is not fixing it.
And again, one does not commit to a particular specialty upon application.
You are wrong, see above.
No, it happens during residency match.
You are wrong, see above.
No, you see above, where I linked to a video about the Residency Match.
Also, in another post you proposed that medical schools should change the residencies if they want more GPs,
Residencies and med schools are separate. And residencies are mostly funded by Medicare, so Congress could expand GP residency slots by increasing funding for them.
but this will obviously not solve the problem as people are not required to stay in the area of their residency after completion, and so the underserved areas will continue to have to replace their healthcare force regularly and at great cost, unless they can select in medical school for applicants who have a passion and a reason to commit to serving these areas.
I do not see how medical schools can control where somebody will work say a decade after graduation.
More GP residency slots would mean more GPs. Yes, residencies do not control where one will work. That can only happen by funding rural medical centers and hospitals and make those positions more attractive.
And you will once again claim that medical schools don’t target specialties upon application and that there’s no reason white or Asian applicants will eschew underserved care at a different rate, as if you had never read an explanation of why that is demonstrably so.
They may target certain specialties. That does not change the fact that specialties are locked in at The Match, not when somebody applies for med school.
And it does not justify discriminating against Asians and whites merely because you think they are less likely to work in underserved areas.